
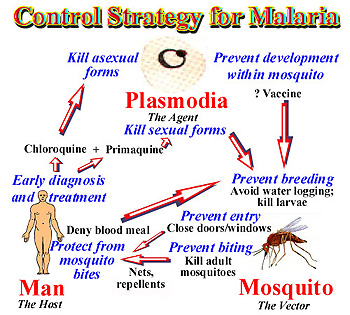
Malaria control
Prevention measures
Prevention of malaria is currently based on two complementary methods: chemoprophylaxis and protection against mosquito bites. While several malaria vaccines are under development, none is available yet.
Chemoprophylaxis
In Europe, malaria chemoprophylaxis is only for travellers to malaria endemic countries, which are classified in three (or four) groups, to determine which drug is recommended for chemoprophylaxis. The choice of drugs depends on the travel destination, the duration of potential exposure to vectors, parasite resistance pattern, level and seasonality of transmission, age and pregnancy. In endemic countries, chemoprophylaxis could also be recommended for autochthonous young children and pregnant women, depending on endemicity level and seasonality of transmission.
Personal protection measures against mosquito bites
Because of the nocturnal feeding habits of most of Anopheles mosquitoes, malaria transmission occurs primarily at night. Protection against mosquito bites include the use of mosquito bed nets (preferably insecticide-treated nets), the wearing of clothes that cover most of the body, and use of insect repellent on exposed skin. Type and concentration of repellents depend on age and status.
Mosquito control
Vector control measures depend on vector species, mosquito biology, epidemiological context, cost and acceptability by populations. The main current measures are focused on reduction of the contact between mosquitoes and humans, the destruction of larvae by environmental management and the use of larvicides or mosquito larvae predators, and destruction of adult mosquitoes by indoor residual spraying and insecticide-treated bed nets.
TREATMENT
For P. falciparum infections acquired in areas with chloroquine resistance, four treatment options are available. These include
Artemether-lumefantrine (Coartemâ„¢), which is the preferred option if readily available.
Atovaquone-proguanil (Malarone™). These are fixed-dose combination therapies that can be used for pediatric patients ≥5 kg.
Quinine sulfate plus doxycycline, tetracycline, or
clindamycin is also a treatment option.
For the quinine sulfate combination options, quinine sulfate plus either doxycycline or tetracycline is generally preferred to quinine sulfate plus clindamycin because there are more data on the efficacy of quinine sulfate plus doxycycline or tetracycline.
No Quinine should be given for 3 days, except for infections acquired in Southeast Asia where 7 days of treatment is required. The fourth option, mefloquine, is associated with rare but potentially severe neuropsychiatric reactions when used at treatment dose. We recommend this option only when the other options cannot be used. In addition, mefloquine is not recommended for infections acquired in certain parts of Southeast Asia due to drug resistance. Once a treatment regimen is started, if it is being tolerated, there is no need to switch regimens even if a preferred regimen becomes available.
Options for treatment of pregnant women are presented in the “Alternatives for Pregnant Women†section below. Due to the risk of progression to severe disease, uncomplicated malaria treatment should be initiated as soon as possible with the regimen that is most readily available. In addition, clinicians should hospitalize patients with P. falciparum infection to monitor clinical response and check parasite density every 12–24 hours. Once clinical presentation improves and a decrease in parasite density becomes apparent, treating clinicians can consider outpatient completion of treatment.
For pediatric patients, the treatment options are the same as for adults except the drug dose is adjusted by patient weight, and artemether-lumefantrine (Coartem™) and atovaquone-proguanil (Malarone™) can only be used in children ≥5 kg. The pediatric dose should never exceed the recommended adult dose. Pediatric dosing with quinine may be difficult due to unavailability of non-capsule forms of this antimalarial. If using a quinine-based regimen for children less than 8 years old, doxycycline and tetracycline are generally not recommended; therefore, quinine can be given in combination with clindamycin as recommended above. In rare instances, doxycycline or tetracycline can be used in combination with quinine in children less than 8 years old if other treatment options are not available or are not tolerated, and the benefit of adding doxycycline or tetracycline is judged to outweigh the risk.
For infections attributed to “species not identified†in areas with chloroquine resistance that are subsequently diagnosed as being due to P. vivax or P. ovale, additional treatment with primaquine or tafenoquine should be administered .

 0
0



.jpeg)


.jpeg)














.jpeg)

.jpeg)
0 Comment(s)